The Corpus Concept
The Corpus Concept is a measuring system for analysing and documenting body posture and motor functions. The documented analysis provides physicians with supportive information for their diagnoses, therapists with a clear therapeutic approach, and helps orthopaedic technicians and shoemakers in the creation of corresponding aids for synergistic support.
The evaluation of the digital posture analysis provides information about the perpendicular distances, angles and curvatures between the body's various segments. These are calculated precisely.
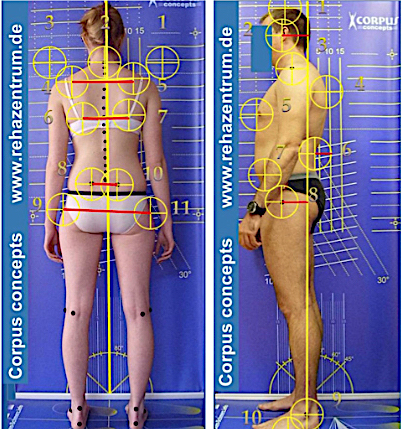
The posture analysis is performed in a digital side, front and back view in front of a measuring wall with a correspondingly high resolution, and an angle plate. The Corpus Concept analysis is based on individual angles and perpendicular distances that are in turn aligned with numerical values which are extant in the medical nomenclature and help with the subsequent assessment of the analysis.
This Corpus Concept check also includes motor function tests enabling an assessment of the patient's balance and coordination skills. The results of an orthopaedic examination and of muscle tests are also similarly recorded in the Corpus Concept.

The Corpus Concept generates an automatic report that supports the therapist in possible therapeutic measures, but also exercises for the patient's daily training. The patient's data and pictures are stored in a data base and will even be available for comparison in many years' time.
The analysis will not only highlight the causes of complaints in the postural apparatus of the back or the mechanical axes, but also of TMJD (temporomandibular joint dysfunction syndrome), thus enabling the therapist to eliminate these complaints by way of suitable therapeutic measures.
It is also particularly suitable for children, as it will track their growth from infancy to adulthood in terms of the mechanical axes and arches. There are also exclusion tests with school satchels and school bags, ensuring that the analysis is also able to provide suitable therapeutic measures for eliminating postural defects.
The analysis of the performed tests is provided to the physician and patient, and in the case of children and adolescents also to their parents.
Bowlegs and knock knees are normal when children grow up
Up to school age, putative misalignments of the legs such as bowlegs, knock knees or inward pointing feet are not abnormal, but usually attributable to delayed growth.
Babies and toddlers always have bowlegs, for instance.
If a one-year old, for example, stands straight with the ankles touching, it will have bowlegs. One can easily pass a broad hand through the gap between the knees.
These bowlegs will usually disappear by the end of the first year of life, but just a year later, children will exhibit strong knock knees, which are only temporary infantile knock knees, however, i.e. an x-shaped alignment of the legs that will pass. The effect on the feet would be highly unfavourable otherwise in the long run. They would need to tilt to the inside to keep the balance.
It will hence be seen that the bowlegs have disappeared by the age of three at the latest, which is not pathological.
The knock knee position will wane in the following years of growth, and by the time of enrolment in school, or by the age of eight at the latest, the strong knock knees will have usually disappeared. A slight physiological knock knee position may remain, so that only 1-2 fingers can now be passed between the insides of the knees when the ankles are touching.
Health checks of children have shown that 80 % of the examined children over ten will have a healthy mechanical axis, while 11 % exhibit a heightened knock knee position, and 9 % bowlegs.
In the latter cases, the disappearance of this misalignment of the mechanical axis should be urgently checked in the later growing periods. The repeated changes of the shape in the development from baby to teenager is also a consequence of the growth of the entire body, a process in which the feet, the pelvis and also the spine are all remodelled.
Scientists hence attribute this conspicuous development of the legs to an own intelligence of the bones.
The bones largely consist of hard braces in a sponge-like structure. In the course of life, this structure develops in a manner ensuring that forces acting from the outside, as experienced when a person is running, jumping, or also falling, will only impact the bones to a minimal extent.
Motion is enabled by way of the muscles, which start and end in sinews at the respective bones. This means that strong muscles apply tensile forces to the bones they are attached to with sinews, providing them with mechanical stimuli that in turn promote their growth. It should hence be ensured that children and adolescents get enough physical exercise, because this is undoubtedly the only way of ensuring that their feet, legs and entire bone structure will enjoy healthy growth.
Scientists at Münster university hospital have highlighted the complexity of this remodelling of the bones until a normal, upright mechanical axis is reached at the age of six. To do this, the scientists involved, Dieter Rosenbaum, Kerstin Bosch and Joachim Gress, studied the children over nine years of their development, starting at the age of 14 months.


Besides growth-related changes in the skeleton, they also found marked changes in the gait (see also the interview with Maximilian Werding in Saaramateur issue …, 20..., where "Tips for training the young, international comparison in top-class sports", be it team sports or individual disciplines, indeed give occasion to think about the training of young talents in German high-performance sports).
Paediatricians tell tales of worried parents who have observed their child's inward-turned gait and hence fear a pathological misalignment. The scientists can very often also provide reassurance in this respect because the angle at which the femoral neck - the part that sticks out to the side at the top of the thighbone - is turned forward in the hip joint will change as a person grows up. With up to 30°, this torsion is still very large in children.
As a consequence, the body turns the leg slightly inward at the hip joint to ensure an optimal fit of the head of the femur in the socket of the hip joint, and thus an optimal burdening of the joint. This is what brings about the inward-turned gait of children.
In the course of growing up, the angle of this torsion will become smaller, so that the body no longer needs to turn the leg to the inside so strongly when walking, and the leg and foot will instead turn slightly outward.
….With children not only lengthwise, but will also turn outward like a corkscrew as they grow.
Up to the age of two, children will initially always walk with strongly inward-turned feet. But the legs will continue turning outward progressively in the years to follow. At the age of 6, the feet are already turned outward by an angle of approximately 5°. And from the age of 12, the hip and lower legs ill have already turned to an extent that the feet face outward by 5°- 15°, if the knee joints are facing straight ahead. The body weight is hence automatically rolled over the ball of the big toe. The final position of the mechanical axis should have become established by the age of 14 in adolescents, at the latest.
Whether this is the case can be checked by the parents themselves: if the child stands upright with the insides of the ankles touching and knees straightened, the distance between the knee joints should approximately equal two finger widths.
But:
Not every deviation is immediately a misalignment or even pathological. We are not cast from moulds, after all, but unique individuals that therefore also grown in their own, individual manner.
 DE
DE
 FR
FR